

|
|
By Richard Gale and Gary Null PhD, Progressive Radio Network
Over the years we have written approximately seventy investigative articles specifically dealing with vaccination, with cited scientific studies, to expose the poor science about vaccine efficacy and safety, blatant misinformation, media propaganda and the politicization of national health policies.
It would take any mainstream journalist a minimum amount of time to gather sufficient research to discover the prima facie evidence behind the CDC’s propaganda to push and mandate massive vaccination campaigns.
There are volumes of investigative reports detailing drug companies’ overwhelming influence on regulatory agencies, flagrant conflicts of interest, and gross negligence to properly evaluate vaccines based upon objective methodological principles.
In the past, CDC officials have perjured themselves before Congress and have engaged in massive cover ups to conceal the dangers of specific vaccines and their ingredients, which are contributing to an epidemic of injuries among America’s infants, children and youth.
The same can be said for the FDA, the Department of Health and Human Services, the American Academy of Pediatrics and other professional medical organizations. Each agency and organization aligns itself with vaccine policies that favor corporate sales and profits at the expense of public health.
Journalists who bother to look will undoubtedly find dozens of board-certified physicians who have individually spent thousands of hours delving into the peer-reviewed medical literature to uncover scientifically sound evidence to challenge the nation’s vaccine policies and the CDC’s childhood vaccination schedule.
However, to do so, journalists out of necessity would need to turn against their handlers, the media’s doctors-for-hire, and corporate advertisers who have captured practically every major newspaper, magazine and multimedia network to circulate one-sided and biased narratives that vaccines are effective and safe.
Sadly, it is a bad career move for an aspiring journalist to be honest and adhere to scientific integrity when accurately reporting about the human cost of vaccination.
Modern vaccinology should not follow a one-size-fits-all theory as the pro-vaccine industry believes. For a coherent medical debate on vaccine safety, it is necessary for each vaccine to be critically evaluated on its own terms. Proper evaluation should include the properties of viral infection and immune response, adverse effects, long term risks that may not present detrimental outcomes until years after inoculation, and discerning the ratio between efficacy benefits against safety risks.
It is dangerous to assume that a new drug or vaccine to fight an infectious disease or life-threatening disease will be safe after it is released upon an uninformed public. The history of pharmaceutical science is a long story of disastrous failures. Numerous drugs over the decades have been approved and later found to be more life threatening than the illnesses being targeted. Unfortunately this is only discovered after countless people have been injured.
Despite efforts to minimize its risks, the whole cell pertussis vaccine was a disaster. Starting in the 1950s, increasing cases of encephalopathy following vaccination resulted in a flurry of lawsuits against the vaccine makers. Eventually the whole cell vaccine was pulled from the market and replaced by a killed acellular alternative. Pharmaceutical companies started to abandon the vaccine market due to rising injury compensation suits and the loss of insurance liability.
After the Reagan administration passed the National Childhood Vaccine Injury Act in 1986, thereby removing the pharmaceutical and biotech companies from medical liability, vaccine development boomed. The combination of removing legal incentives to perform robust clinical trials to ascertain vaccines’ safety profiles, and the gradual reduction of honest and rigorous evaluation by federal authorities, has provided vaccine makers a free pass to rush vaccines through the CDC and FDA approval process with shoddy research.
The first human papilloma vaccine (Merck’s Gardasil) is an excellent example of a post-1986 vaccine that fundamentally holds no benefits over and beyond safer interventions to prevent the progression of HPV infections.
Private vaccine developers have free license to test and evaluate new drugs and vaccines inadequately if they wish. They also have the freedom to manipulate trial data to derive a lucrative outcome. Yet, ultimately, whether their products reach the market or not depends upon the CDC’s and FDA’s oversight.
Our health agencies are mandated by Congress to protect and serve the improvement of public health rather than corporate interests and profits. Consequently, the buck stops with the federal health authorities and those who appoint them whether or not an efficacious and safe vaccine is approved. However, by allowing themselves to be increasingly hijacked by private pharmaceutical interests, our health agencies have turned into a self-serving culture chronically deceiving the public.
Today distrust in the government and the medical establishment has never been so high. In late 2020, according to the Alliance for a Stronger FDA, only 8 percent of Americans had strong trust in the FDA. Forty two percent said they had very little or no trust at all.
During the pandemic, the CDC fared no better at approximately 50 percent; however, overall only 34 percent believed our nation’s health system was capable of protecting the public.
Confidence in NIAID’s Anthony Fauci’s handling of the pandemic has plummeted to 31 percent, according to a Quinnipiac University poll, compared to over 80 percent a year prior. Recent loss of trustworthiness undoubtedly parallels decreasing compliance in people receiving boosters. And a Kaiser Family Foundation survey found that only 27 percent of parents were eager to have their children vaccinated.
As more Americans lose faith in government over the failure of their policies, lack of leadership and false promises, crucial human rights issues are being raised. The number of physicians who acknowledge mRNA vaccines’ high risks is escalating.
On-the-ground medical personnel working in clinics and hospitals know firsthand that the vaccines are not preventing the spread of the virus.
People feel betrayed because they have been lied to. Opposition to the Covid-19 vaccines and especially compulsory vaccination for jobs and attendance to colleges and schools will continue to rise as more people fall victim to vaccine injury and deaths, particularly in young adults and soon children will mount. No informed consent is given to people wishing to be vaccinated, nor are they advised about potential adverse side effects. Yet this has almost always been the case throughout the history of vaccination.
Arguably this is a violation of the Nuremberg Code. The conclusions of the Nuremberg Tribunal unequivocally state that “voluntary consent of the human subject is absolutely essential” and individuals should “be able to exercise free power of choice, without the intervention of any element of force, a, deceit, duress or other ulterior forms of constraint or coercion.” In addition, people must be provided with “sufficient knowledge and comprehension of the elements of the subject matter involved as to enable them to make an understanding and enlightened decision.”(Nuremberg Tribunal 1949, pp 181).
None of the terms of the Tribunal have been met during the course of massive vaccination and booster campaigns. Consequently, based upon the wording of the Tribunal’s medical ethics, and the subsequent Helsinki Declaration, our federal health agencies and state legislatures, which seem determined to impose mandates, can technically be accused of similar but lesser crimes.
Most of the growing number of physicians who oppose the Covid-19 vaccines regularly remark that they are not anti-vaccination. They only dispute the government’s claims about the Covid vaccines, in particular those engineered by Moderna and Pfizer. On the other hand we are also witnessing more physicians who clearly recognize the culture of corruption at the highest levels of the CDC, FDA and Anthony Fauci’s NIAID starting to question the government’s claims about other vaccines.
Our health authorities use the same arguments against professional opposition that have been used for decades against critics of the pre-Covid vaccines for measles, influenza, hepatitis, pertussis, HPV, and others. In unison they tout robust vaccine efficacy to prevent infection and transmission; that vaccines are overwhelmingly safe except in very rare instances; and, massive vaccination compliance is a national necessity in order to reach herd immunity and thereby eradicate a virus or bacteria altogether. These are three areas to be investigated with respect to other non-Covid-19 vaccines.
If the government is willing to cut every corner in order to bypass many standard evaluation reviews to hustle experimental genetically engineered vaccines, which have never before been administered to entire populations, why should we not suspect this gross disregard for public safety dates back to the Reagan administration and the 1986 vaccine bill?
There is plenty of documented evidence that this is the case, especially since the mid-1990s when rates of autism skyrocketed and later when the CDC made effort to conceal evidence that overly vaccinated children starting at infancy may be the cause. Nevertheless, we need to investigate each major vaccine on its own terms in order to derive a broader overview of the flaws and failures of the entire vaccination regime as a whole.
Human Papillomavirus (Gardasil)
The CDC’s vaccine adverse reporting system, VAERS, is frequently criticized for being terribly inefficient and cumbersome. There are no obligations for doctors, hospitals and clinics to record potential vaccine-induced injuries or deaths into the system. Consequently many healthcare professionals don’t know it even exists. For that reason, only a small fraction of vaccine injuries and deaths, perhaps as low as 2 percent according to early Harvard University study, ever get reported to federal health officials.
Despite its many shortcomings, ever since the launch of VAERS, the CDC has consistently failed to improve and correct VAERS. Without accurate case data about vaccines’ adverse effects, it is impossible for federal health authorities, as well as independent medical researchers, to properly assess vaccinations’ real risks.
Nevertheless, after looking at the data recorded in VAERS, the Covid-19 vaccines overwhelmingly represent the majority of vaccine-related injuries and deaths. Following the Covid-19 vaccines, and especially Pfizer’s and Moderna’s mRNA vaccines, the HPV vaccine is the next most lethal.
Merck’s human papillomavirus vaccine Gardasil is a classic example of a post-1986 vaccine that carries all of the faults and commercial manipulation solely for profit rather than to improve public health. Aside from Gardasil no other vaccine has been tested under proper inert placebo-controlled studies.
The average person tends to think of vaccines and pharmaceutical drugs as two separate categories. Many nations on the other hand categorize vaccines’ safety profiles similar to other drugs.
Was a vaccine tested to determine fetal and maternal safety? Was it tested for any potential carcinogenic activity? The majority of vaccines on the market have not been tested for either. In addition, unlike common over the counter and prescription medications, vaccines are rarely ever tested against an inert placebo such as a saline solution. In the absence of such rigid safety trials, it becomes virtually impossible to draw solid medical conclusions about a vaccine’s true safety profile and the likely rates of adverse effects.
Before receiving FDA approval, the HPV vaccine Gardasil was tested on fewer than 1,200 girls. Subsequent trials included many more participants. However, in the early trials only 27 percent of the enrolled girls were actually administered the complete three-vaccine series. Another remarkable misstep in the trials was that no girls under age 15 participated, despite the fact that today the vaccine is administered to girls starting at age 9. Nevertheless, the vaccine was fast tracked by the FDA in 2006. Rushing Gardasil through the regulatory hurdles was gross negligence. Seventeen girls died before and after the trial; nevertheless without any compelling evidence the CDC states none of these deaths were due to the vaccine.
Merck’s methodology during Garadsil’s pre- and post-licensure trials was reviewed in a 2012 analysis by scientists at the University of British Columbia and published in the journal Current Pharmaceutical Design. The research team didn’t mince words in their assessment of the trials’ flaws:
“We carried out a systematic review of HPV vaccine pre- and post-licensure trials to assess the evidence of their effectiveness and safety. We found that HPV vaccine clinical trials design, and data interpretation of both efficacy and safety outcomes, were largely inadequate. Additionally, we note evidence of selective reporting of results from clinical trials (i.e., exclusion of vaccine efficacy figures related to study subgroups in which efficacy might be lower or even negative from peer-reviewed publications). Given this, the widespread optimism regarding HPV vaccine’s long-term benefits appears to rest on a number of unproven assumptions (or such which are at odds with factual evidence) and significant misinterpretation of available data.”
Early doubts about the FDA’s approval of Gardasil came from an unlikely source, Dr. Diane Harper, a consultant for Merck and the chief scientist overseeing the clinical trials to evaluate Gardasil’s safety and efficacy. After receiving FDA approval, Dr. Harper publicly questioned Gardasil’s efficacy and public health value compared to the successes in preventing HPV infections from conventional PAP smears.
Among her concerns was that no data showed that Gardasil remains effective after 5 years. A truly effective HPV vaccine, on the other hand, would need to be efficacious for a minimum of 15 years in order to prevent cervical cancer. And that too is misleading. The median age for early cervical cancer diagnosis is 50 and cervical cancer’s median age for death is 58. Furthermore, cervical cancer only represents less than 3 percent of all cancers and approximately one one-hundredth of the U. S. population.
Yet, the CDC targets children who have negligible cervical cancer risk.
Gardasil sales continue to increase globally.
In addition, Dr. Harper estimated that every American 11 year old girl would have to be vaccinated for the next 60 years in order to have any measurable effect on rates of cervical cancer. Scientists from the University of Texas presented research at a meeting of the American Association for Cancer Research revealing that vaccinated women were at a significantly higher risk to become infected with HPV strains not contained in the vaccine when compared to unvaccinated women.
Another study published in the Journal of the American Medical Association (JAMA) demonstrated the ineffective nature of Gardasil in women with existing HPV infections. The authors concluded that Gardasil offers no benefit to women recovering from HPV during a 12-month period. The research team stated that they “see no reason to believe that there is therapeutic benefit of the vaccine elsewhere because the biological effect of vaccination among already infected women is not expected to vary by population.”
In fact, a paper out of the University of California at Berkeley and appearing in Molecular Cytogenetics suggests that cervical cancer may not be caused by the human papilloma virus. If the theory is correct then the HPV vaccines are utterly useless.
Ninety percent of all HPV cases disappear within 2 years. Cervical cancer is highly curable when detected early. The regular use of pap smears have helped decrease the incidence of cervical cancer in the United States by over 50% since the 1970s. Examining health data from Finland and the U.K., Dr. Harper and her colleagues concluded that HPV vaccinations give a false sense of security to many young women and girls who in turn opt out of regular pap smear tests. According to Dr. Harper, this trend has resulted in exponential increases in recent HPV rates.
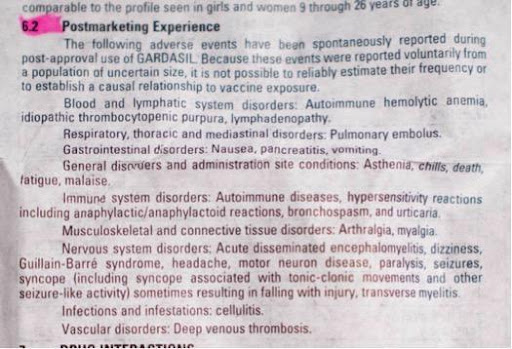
Aside from a limited and medically viable reason for vaccinating against HPV, Gardasil has been associated with a long list of serious adverse effects and many are life-threatening.
The National Vaccine Information Center, a watch-dog organization investigating vaccine injury trends and federal policies, reported that
“After the original Gardasil vaccine was licensed for 11-12 year old girls and young women, thousands of adverse reaction reports were filed for: sudden collapse with unconsciousness within 24 hours, seizures, muscle pain and weakness, disabling fatigue, Guillain-Barre Syndrome (GBS), facial paralysis brain inflammation, rheumatoid arthritis, lupus, blood clots, premature ovarian failure, optic neuritis, multiple sclerosis, strokes, heart and other serious health problems, including death. Similar reports have been filed for the Gardasil-9 vaccine…”
By the end of 2019, the federal Vaccine Adverse Event Reporting System (VAERS) had received over 62,000 cases of adverse reactions from the HPV vaccine, including 503 deaths, over 6,200 hospitalizations and over 3,000 disabling injuries. Forty-seven percent of these vaccine injuries occurred in children and teens between 12-17 years of age. Despite the large number of injury and death claims associated with Gardasil that have been filed to the federal vaccine injury compensation court, less than a third have been accepted with victims being compensated.
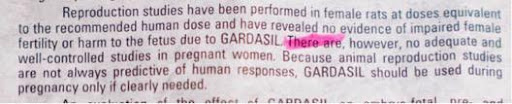
Moreover, Gardasil’s manual insert for physicians states it has not been adequately tested to determine whether it impairs a woman’s fertility or harms the fetus.
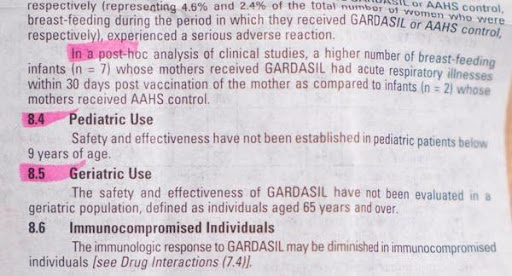
Breastfeeding infants whose mothers have received Gardasil have a high chance of coming down with acute respiratory distress.
Finally, by whatever means, private independent physicians, pathologists and researchers worldwide have been getting possession of vials of Pfizer’s and Moderna’s mRNA vaccines. Investigating the contents of the vials under high magnification dark and light microscopy, their discoveries have been startling and worrisome.
Unusual unidentified nano-chemical structures are being observed that have no correlation to vaccines’ ingredients as published by the drug companies. The verdict is still out about what these ingredients are and why. However, this happens to have a parallel with Gardasil.
In 2018, Italians took to the streets in a massive protest against a mandatory vaccination law. The anger concerned an independent Italian laboratory Corvelva that studied the contents in seven vaccines, including Gardasil. Their findings led to a national scandal that became known as “vaccinegate” as ingredients were discovered to be quite different from what Merck reported to Italian health officials.
Gardasil-9 was loaded with foreign bacterial DNA, which accounted for 54 percent of the vaccine’s total DNA, including human and mouse DNA. Out of 338 different contaminants found, only 22 percent could be identified. In addition, although the vaccine was supposed to protect against 9 different HPV strains, only 7 antigen strains were found in the vials analyzed.
If the vaccine manufacturers intend to be transparent and voluntarily inform the public as to every vaccine ingredient, then they will deserve our trust.
Nevertheless, obfuscation is highly profitable. Merck reported a 36 percent revenue increase reaching $1.6 billion between 2021 and 2022. After factoring in Merck’s profit boom, is it reasonable to believe that national and state health authorities’ efforts to mandate Gardasil into the vaccination schedule has nothing to do with protecting public health?
The views and opinions expressed in this article are those of the author[s] and do not necessarily reflect the views of The Trends Journal.